 Survivalist Pro
Survivalist Pro
Survivalist Pro
Survivalist Pro

 Photo: Mikhail Nilov
Photo: Mikhail Nilov
CPR should be performed immediately on any person who has become unconscious and is found to be pulseless.

A 3-day cleansing diet is a short-term diet plan that focuses on consuming whole and natural foods to help detoxify the body. It typically includes...
Read More »
Their ages of death were compared to men listed in the more recent Chambers Biographical Dictionary. Of 397 ancients in total, 99 died violently by...
Read More »
One main reason is that we are so accustomed to and easily habituate to our environment, and in some ways that can help us focus. For example, you...
Read More »
A 1930s dinner party menu would probably also have included dishes that mirrored what Hollywood considered sophisticated European taste with items...
Read More »
The answer is yes, but not without some difficulties. Firstly, unclaimed islands are usually unclaimed for a reason. The US retains 12 islands...
Read More »
No wonder it's often called the ultimate survival food. Rice. ... Dried Beans. ... Spices. ... White vinegar. ... Canned Foods. ... Bouillon Cubes....
Read More »
Survival tools on the list include a hatchet, climbing rope, a hammock, fishing line and a pocket knife. Contestants can even bring a couple items...
Read More »
Common warning signs of emotional distress include: Eating or sleeping too much or too little. Pulling away from people and things. Having low or...
Read More »
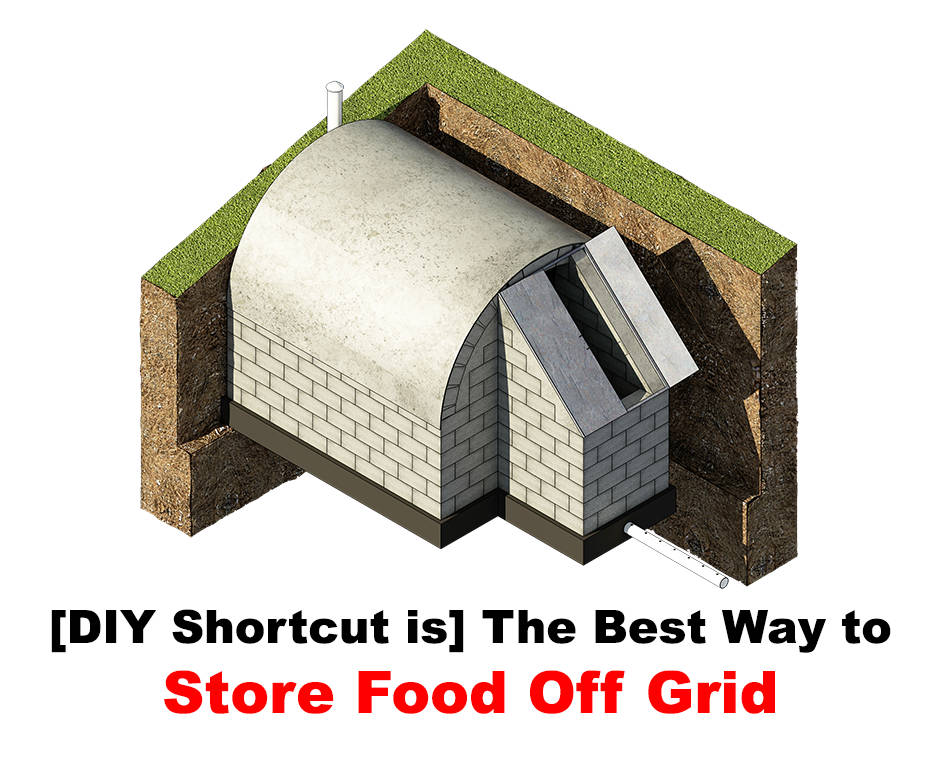
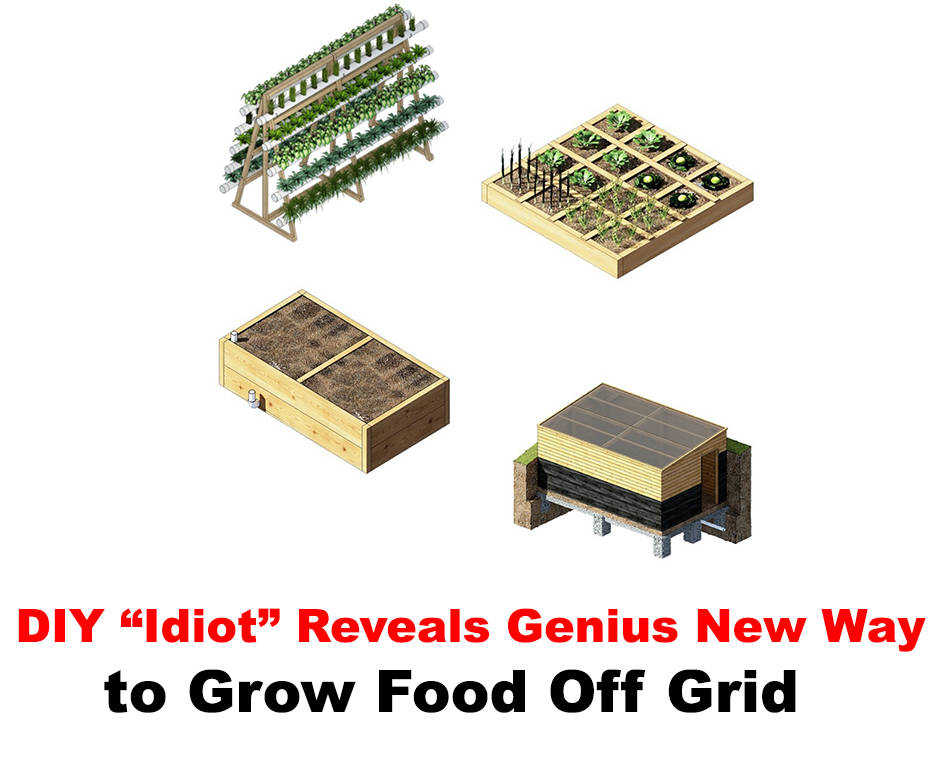
not using public supplies of utilities such as electricity, water, etc. Oct 21, 2009
Read More »
It's best to avoid placing our gun safes in the garage, but if there is no other choice, it's a good practice to bolt it to the floor and build a...
Read More » Promotion
Promotion
 Promotion
Promotion
 Promotion
Promotion
 Promotion
Promotion